| |
| |
| Kidney (Renal) Transplantation |
|
|
Kidney transplantation is one of the most common and successful organ transplant procedures performed today. Thanks to decades of fine-tuning, renal transplantation has become a life-saving alternative for thousands of patients with end-stage renal disease.
For patients with kidney failure and those who are not candidates for transplantation, dialysis can sustain life. But what can you expect from either option? The information below can help you discuss renal treatment with your urologist. |
| |
|
What happens under normal conditions? |
|
|
The kidneys are fist-sized organs responsible for the fluid and chemical balances of your body. Located on both sides of the spine behind the liver, stomach, pancreas and intestines, these two organs are protected by the lower ribs and muscles of the back and sides.
When healthy, your kidneys cleanse the blood of waste products and produce urine. They also balance essential elements, such as sodium and potassium, while providing hormones necessary to regulate blood pressure and red blood cell production.
When these organs fail, harmful wastes build up in your body, leading to high blood pressure, increased fluid retention, imbalances in salts and acids in the blood, and decreased red blood cell production. All of those events can have harmful, possibly life-threatening effects on your heart and brain. |
| |
|
What causes kidney failure? |
|
|
| Each year about 90,000 Americans develop end-stage renal disease. The most prevalent causes of chronic kidney failure include diabetes, high blood pressure and glomerulonephritis, an inflammation of the organ's filtering units. These conditions account for three-quarters of reported end-stage cases. |
| |
|
What are the symptoms of kidney failure? |
|
|
There are many symptoms associated with kidney failure. You may experience swelling in your hands, feet and face along with headaches due to high blood pressure, and even seizures. Your complexion may pale due to anemia, and your urine may become coffee-colored. You may also have chronic bad breath that cannot be freshened by brushing your teeth. You may have fatigue and itchy skin. |
| |
|
How is kidney failure treated? |
|
|
The most common treatment for end-stage kidney disease is dialysis. This is the process of removing waste, excess water and chemicals (e.g., potassium, sodium, calcium and acid) from the body. There are two types of dialysis: hemodialysis and peritoneal dialysis.
In hemodialysis, the patient's blood stream is connected to an artificial kidney machine outside the body. Hemodialysis treatments are usually done three times per week and take from two to six hours for each session. Many patients with kidney failure undergo peritoneal dialysis, a similar cleansing process conducted through a tube in the abdomen.
While hemodialysis and peritoneal dialysis will not cure kidney failure, they can replace the work of your kidneys, helping you feel better and live longer.
About 30 percent of kidney failure sufferers are suitable candidates for a kidney transplant, a surgical procedure to restore function by replacing two failed kidneys with one healthy organ.
About half of kidney transplants come from non-living (or deceased) donors, even though family members, spouses (living, related donors) and friends (living, unrelated donors) can safely donate if tests can prove they'll have nearly normal kidney function after giving up one kidney.
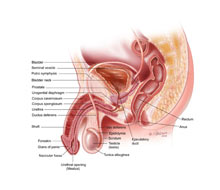
A kidney transplant is usually placed in the lower abdomen without any need to remove the failed kidneys. The new kidney's artery is connected to one of the patient's pelvic arteries. The kidney's vein is connected to one of the veins in the patient's pelvis. The ureter, the tube that drains urine from the kidney, is connected to the bladder or to one of the patient's own ureters. In children, the blood vessels from a large adult kidney transplant are frequently connected to the child's aorta and inferior vena cava. |
| |
|
What can be expected after treatment for kidney failure? |
|
|
If you are the donor, you can expect to leave the hospital between two to four days after the surgery. If your kidney was removed with a traditional operation, expect a single incision about eight inches in length. If, however, your doctor has used laparoscopic surgery, a minimally invasive procedure, you will have four smaller incisions, the largest of which will be about four inches long.
If you are the recipient of the transplant, you will have a catheter in your bladder and an intravenous feeding tube through your arm and/or neck vein for a few days after the procedure. You can expect to be up, out of bed and walking within 24 hours and discharged in five to seven days. While urine often flows immediately, sometimes the new kidney does not work effectively right away. So do not be surprised if you need temporary dialysis.
About 90 percent of transplanted kidneys are functioning at the end of one year. Between 3 percent to 5 percent of these kidneys stop working each year after that. The kidney is always at risk for rejection, so it is very important for kidney transplant patients to take all of their medicines as directed to prevent this problem. Overall, a kidney from a living donor has a better survival rate than a kidney from a non-living donor.
The chance that you will have a recurrence of kidney disease in your transplant depends on the cause of your kidney failure. For instance, it does not occur with autosomal dominant polycystic kidney disease, or other inherited disorders. It is possible with conditions such as hemolytic uremic syndrome, a rare disorder marked by kidney failure, or focal segmental glomerulosclerosis, a severe disease in which scar tissue replaces the kidney's filtering glomeruli. |
| |
|
| |
| Frequently asked questions: |
| |
What are the risk factors for kidney failure? |
|
|
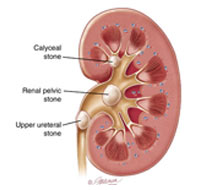
Any number of risk factors can contribute to kidney failure including high blood pressure, hardening of the arteries and diabetes. It can be brought on by untreated strep infections, recurrent and chronic kidney infections, systemic lupus erythematosus, severe forms of diarrhea, kidney stones or even chronic use of non-steroidal anti-inflammatory drugs. |
| |
|
I'd like to donate one of my kidneys to my brother but our blood types are not identical. Does it matter?
|
|
|
No. Blood types do not have to be identical, just compatible. Markers or "antigens" on the surfaces of your red blood cells determine your type.
ABO blood group incompatibility between the donor and recipient can provoke an immediate rejection. This means that a donor with "O" blood type can donate a kidney to a patient who has "O," "A," "B" or "AB" blood type and that transplant candidates with "A" or "B" blood types are usually limited to kidney transplants from donors with the same blood type or "O" blood type.
Antibodies, proteins manufactured by the immune system that react specifically to donor tissue. A "negative cross-match" or lack of reaction when blood samples from a donor and recipient are test tube mixed confirms when a kidney is acceptable. |
| |
|
| |
How long will I have to wait for a kidney transplant if I do not have a living donor? |
|
|
The waiting period for a deceased donor kidney varies from patient to patient, depending most on patient blood group and degree of antibodies in the blood. Since there are not enough deceased donor organs for every person who needs a transplant, potential recipients are placed on a national list, administered by the United Network for Organ Sharing (UNOS), a private nonprofit organization contracted by the federal government.
Each time an organ becomes available, a recipient is chosen based on a point system reflecting blood type, waiting time, tissue match and antibody levels. Although some people receive their organ within several months, the median delay is two to three years. In contrast, a living-donor transplant can be scheduled immediately, thus making it an optimal choice. |
| |
|
My father had autosomal dominant polycystic kidney disease. What is the chance that I will have the same disease? |
|
|
The chance that you have inherited this condition is about 50 percent. Autosomal dominant polycystic kidney disease should not be confused with multiple simple cysts of the kidneys, which occur commonly with age. Instead, this disease results in a build-up of benign growths that gradually increase in size until they destroy the normal tissue of both kidneys.
Symptoms like abdominal swelling, pain, bloody urine and frequent urinary tract infections may occur at any time but they usually begin in middle age. High blood pressure and renal failure may result as the disease progresses. Although there is no effective treatment to preserve kidney function in patients with autosomal dominant polycystic kidney disease, dialysis or a kidney transplant can be used to treat the kidney failure
|
| |
|
| |
|
|